

We live in a culture where people will swallow, snort, inject, or chug just about anything if it promises to make them happier, sharper, or stronger. Some of it works, some of it doesn’t, and some of it lands you in a congressional hearing.
SSRIs
SSRIs are the antidepressants like fluoxetine, sertraline, escitalopram. They’ve been around long enough to be studied to death1. The verdict is that they’re safe long-term2. Your brain isn’t going to melt, and there’s no hidden timer where they suddenly stop working and ruin your life.
The catch is side effects. Sexual side effects are common3, and in some unlucky cases they linger even after stopping. This is officially called Post-SSRI Sexual Dysfunction4, which sounds like the name of the worst punk band in history. And if you quit SSRIs too fast, your nervous system throws a party you didn’t ask for: dizziness, brain zaps, flu-like misery. Usually temporary, but enough to convince you that tapering is not optional5.

Amphetamines
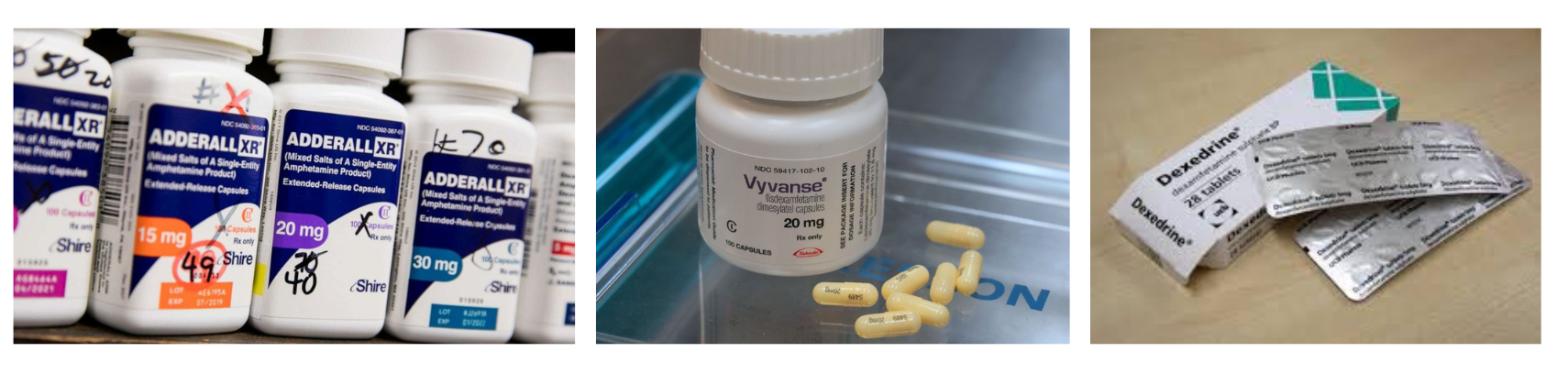
Amphetamines are the ADHD meds with names like Adderall, Vyvanse, Dexedrine. They jack up dopamine and norepinephrine so your brain can focus for longer than ten seconds6. People always worry that long-term use will fry your dopamine system like meth. Spoiler: it doesn’t. Decades of research show that therapeutic doses don’t cause brain rot or permanent depletion7.
In fact, kids with ADHD who take stimulants are less likely to abuse drugs later8, probably because they’re not busy self-medicating with weed and Monster Energy. Stimulants can slow growth in kids by maybe an inch, but most catch up9. When you stop them, you might feel tired or flat for a while, but that fades. It’s more like a long Red Bull crash than a permanent state of doom10. As the I’ve Had It podcast would say, “I’ve had it with people acting like Adderall is meth with a prescription label.”
Caffeine: The OG Pre-Workout
Caffeine is the original performance enhancer. People have been chasing that buzz forever. In the 1904 Olympics, marathon runners were literally dosed with brandy mixed with strychnine11. By the 1930s, caffeine pills were everywhere12. Weightlifters in the 70s swore by black coffee before training, and in the 80s we got Ultimate Orange, a pre-workout that mixed caffeine with ephedra and hit like a freight train13. It worked, until people started having heart attacks, and the FDA banned ephedra14.
Modern pre-workout powders are basically caffeine in a neon tub, sometimes spiced up with beta-alanine (the tingle stuff) and creatine. Is it necessary? Absolutely not. Caffeine does improve performance15, but you can get the same boost from a cup of coffee. The difference is whether you want your caffeine with marketing or not. Pre-workout is psychological as much as physiological. If you believe the scoop will turn you into The Rock, you’ll probably lift harder. If you’re anxious, it’ll just make your heart race faster and convince you you’re dying.
Testosterone, Steroids, and HGH: Bigger Biceps, Smaller Testicles
Synthetic testosterone was first isolated in the 1930s16, and by the 1950s weightlifters and bodybuilders were already injecting it17. Testosterone itself is the natural hormone that makes muscles grow, voices drop, and teenagers unbearable.
When people talk about “anabolic steroids,” they’re usually talking about synthetic derivatives of testosterone that crank up the muscle-building (anabolic) effects while trying to minimize the androgenic ones18. Human growth hormone, or HGH, is in a different category. It was discovered in the mid-20th century19 and originally used for kids with stunted growth20. In adults, HGH increases muscle mass, reduces fat, and makes celebrities claim they’re aging in reverse21.
So what’s the difference? Testosterone is the natural hormone that men and women both make. Anabolic steroids are its lab-designed cousins, tweaked for maximum gains, often at the cost of your liver and your mood22. HGH isn’t testosterone at all. It’s a separate hormone that tells your body to grow everything, not just muscles, which is why too much of it can make your jaw, hands, and heart enlarge23. People use all three because humans love shortcuts, but the risks range from “annoying acne” to an enlarged heart.

The Real Risk
So what happens long-term? With SSRIs, the worry is lingering sexual dysfunction, but that’s rare. With amphetamines, the worry is dopamine burnout, but the research says it doesn’t happen at prescribed doses. With caffeine, the worry is mostly that you’ll become the guy at the gym who spends $60 on a tub of pink powder when a double espresso would have done the same thing. With testosterone, steroids, and HGH, the worry is that your shortcut to bigger biceps will also give you shrunken testicles, mood swings, heart problems, and a lifetime membership in the “why did I do this to my liver?” club24.
The real danger isn’t these substances destroying you later, but untreated depression, untreated ADHD, untreated exhaustion, and untreated insecurity wrecking you right now. Or, as George Carlin would put it: “It’s never just about the medicine. It’s about the culture, the fear, and the bullshit we build around it.”25 If you have a comment, or want to continue this conversation, please contact me through my website: www.boulderpsychiatryassociates.com.
Footnotes
- Wong, D.T., et al. “A new inhibitor of serotonin uptake: LY110140, 3-(p-trifluoromethylphenoxy)-N-methyl-3-phenylpropylamine.” Life Sciences, 1974. ↩
- Cipriani, A., et al. “Comparative efficacy and acceptability of antidepressants in the acute treatment of major depression.” Lancet, 2009, pp. 746–758. ↩
- Montejo, A.L., et al. “Incidence of sexual dysfunction associated with antidepressant agents.” Journal of Clinical Psychiatry, 2001. ↩
- Bala, A., Nguyen, H.M.T., and Hellstrom, W.J.G. “Post-SSRI Sexual Dysfunction: A Literature Review.” Sexual Medicine Reviews, 2018. ↩
- Fava, G.A., and Gatti, A. “Withdrawal symptoms after selective serotonin reuptake inhibitor discontinuation.” Journal of Clinical Psychopharmacology, 2015. ↩
- Heal, D.J., et al. “Amphetamine, past and present—a pharmacological and clinical perspective.” Journal of Psychopharmacology, 2013. ↩
- Volkow, N.D., et al. “Effects of therapeutic doses of oral methylphenidate on dopamine transporter blockade in adults with ADHD.” Journal of Nuclear Medicine, 1998. ↩
- Wilens, T.E., et al. “Does stimulant therapy of attention-deficit/hyperactivity disorder beget later substance abuse?” Pediatrics, 2003. ↩
- Swanson, J.M., et al. “Effects of stimulant medication on growth rates across 3 years in the MTA follow-up.” Journal of the American Academy of Child & Adolescent Psychiatry, 2007. ↩
- Spencer, T.J., et al. “Withdrawal effects after stopping long-term stimulant therapy.” Journal of Attention Disorders, 2006. ↩
- Marks, Harry. The Progress of Experiment: Science and Therapeutic Reform in the United States, 1900–1990. Cambridge University Press, 1997. ↩
- Smith, M.E. “Caffeine: Historical and clinical perspectives.” Journal of Clinical Pharmacology, 2002. ↩
- Yesalis, Charles E. Anabolic Steroids in Sport and Exercise. Human Kinetics, 2000. ↩
- Food and Drug Administration. “FDA announces rule prohibiting sale of dietary supplements containing ephedrine alkaloids.” FDA, 2004. ↩
- Ganio, M.S., et al. “Evidence-based approach to ergogenic effects of caffeine.” Journal of Strength and Conditioning Research, 2009. ↩
- Butenandt, A., and Hanisch, G. “Über die Umwandlung des Dehydroandrosterons in Androstendiol und Testosterone.” Chemische Berichte, 1935. ↩
- Todd, Terry. “Anabolic steroids: The gremlins of sport.” Journal of Sport History, 1987. ↩
- Kicman, A.T. “Pharmacology of anabolic steroids.” British Journal of Pharmacology, 2008. ↩
- Raben, M.S. “Treatment of a pituitary dwarf with human growth hormone.” Journal of Clinical Endocrinology and Metabolism, 1958. ↩
- Rudman, Daniel, et al. “Effects of human growth hormone in men over 60 years old.” New England Journal of Medicine, 1990. ↩
- Liu, H., Bravata, D.M., et al. “Systematic review: The safety and efficacy of growth hormone in the healthy elderly.” Annals of Internal Medicine, 2007. ↩
- Pope, Harrison G., et al. The Adonis Complex: The Secret Crisis of Male Body Obsession. Free Press, 2000. ↩
- Colao, Annamaria, et al. “Systemic complications of acromegaly: epidemiology, pathogenesis, and management.” Endocrine Reviews, 2004. ↩
- Haupt, H.A., and Rovere, G.D. “Anabolic steroids: a review of the literature.” American Journal of Sports Medicine, 1984. ↩
- Carlin, George. Napalm and Silly Putty. Hyperion, 2001. ↩
